
Metotrexato en condromatosis sinovial: una serendipia
Resumen
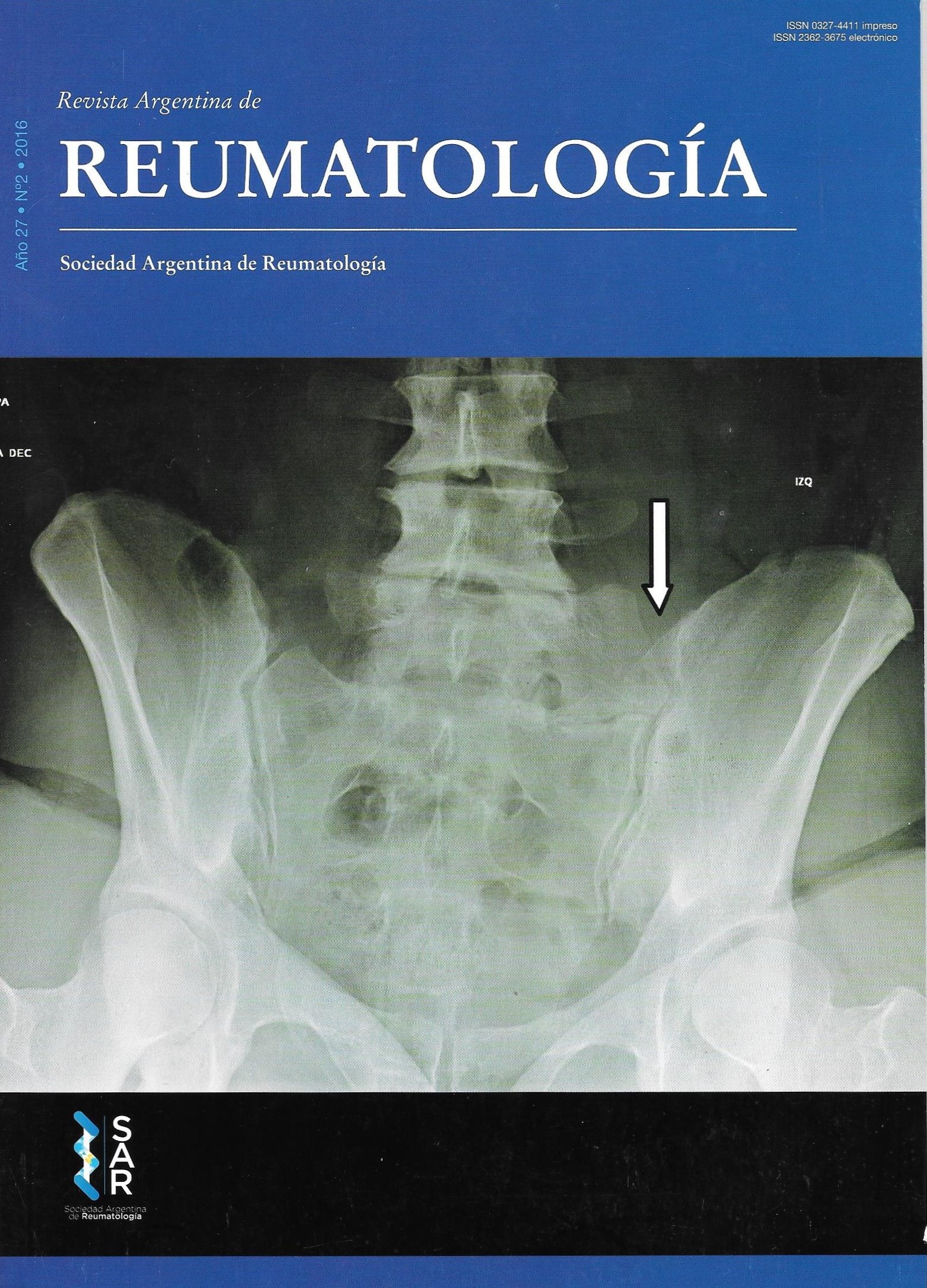
La condromatosis sinovial es una metaplasia idiopática benigna de la membrana sinovial que afecta a 1/100.000 habitantes, en una relación hombre/mujer de 3 a 1 entre los 30 y 50 años. Predomina en grandes articulaciones como rodilla (70%), cadera (20%) y hombro (19%), y en menor proporción en codo y tobillo. Puede ser primaria o secundaria. La etiología es desconocida. La resolución es quirúrgica ya sea por artroscopia o por cirugía a cielo abierto, no existiendo otra alternativa terapéutica. Se presenta el caso clínico de un paciente con condromatosis sinovial en hombro derecho, que se comporta como una artropatía erosiva, indicándose metotrexato y resolviendo casi totalmente los nódulos condromatosos.Citas
I. Jiménez-Martín A. et al. Reumatol Clin. 2014; 10(6):416-417.
II. Milgram JW. Synovial osteochondromatosis: A his-tological study of thirty cases. J Bone Joint Surg Am. 1977; 59:792-801.
III. Gómez-Rodríguez N et al. Condromatosis sinovial. Es-tudio de 39 pacientes. Reumatol Clin. 2006; 2(2):58-63.
IV. Robinson D. et al. Int. Synovial chondromatosis: the possible role of FGF 9 and FGF receptor 3 in its patho-logy. J Exp Path. 2000; 81:183-189.
V. Sato J, Segami N, Suzuki T, Yoshitake Y, Nishikawa K. The expression of fibroblast growth factor-2 and fibro-blast growth factor receptor-1 in chondrocytes in syno-vial chondromatosis of the temporomandibular joint. Report of two cases. Int J Oral Maxillofac Surg. 2002; 31:532-536.
VI. Duymus TM, Yucel B, Mutlu S, Tuna S, Mutlu H, Komur B. Arthroscopic treatment of synovial chon-dromatosis of the shoulder: A case report. Ann Med Surg (Lond). 2015 May 11; 4(2):179-82. doi: 10.1016/j. amsu.2015.05.001. eCollection 20.
VII. Lorusso G, Sarma D, Sarwar S. Pathologic Quiz Case: Soft tissue calcifications of the shoulder in a 31 year-old woman. Arch Pathol Lab Med 2004;128(12):1455-1456.
VIII. Miranda J, Hooker S, Baechler M, Buerkhalter W. Synovial Chondromatosis of the shoulder and biceps tendon sheath in a 10- year-old child. Orthopedics 2004;27(3):321-323.
IX. Campeau N, Lewis B. Case report: Ultrasound appea-rance of synovial osteochondromatosis of the shoulder. Mayo Clin Proc 1998;73(11):1079-1081.
X. Ko E, Mortimer E, Fraire A. Extraarticular synovial chondromatosis: Review of epidemiology, imaging stu-dies, microscopy and pathogenesis, with a report of an additional case in a child. International Journal of Sur-gical Pathology 2004;12(3): 273-280.
XI. Mohr W. Is synovial osteo-chondromatosis a prolife-rative disease?. Pathol Res Pract 2002;198(9):585-589.
XII. Peetrons P, Court-Payen M. Interventional procedu-res in musculoskeletal ultrasound. Seminars in inter-ventional radiology, musculoskeletal interventional. Radiology 2002;19(3):189-196.
XIII. Lieger O, Zix J, Stauffer-Brauch EJ, Iizuka T. Synovial chondromatosis of the temporomandibular joint with cranial extension: a case report and literature review. J Oral Maxillofac Surg 2007;65:2073-80.
XIV. Hecht D, Zimmerman N, Bedford M, Avivi A, Yayon A. Identification of fibroblastic growth factor 9 (FGF9) as a high affinity, heparin dependent ligand for FGF receptors 3 and 2 but not for FGF receptors 1 and 4. Growth Factors 1995;12:223-33.
Derechos de autor 2016 Sociedad Argentina de Reumatología

Esta obra está bajo licencia internacional Creative Commons Reconocimiento-NoComercial-SinObrasDerivadas 4.0.




